INNOTEST® β-AMYLOID(1-42)
The INNOTEST β-AMYLOID(1-42) is a solid-phase enzyme immunoassay for the quantitative determination of β-amyloid(1-42) in human cerebrospinal fluid (CSF).
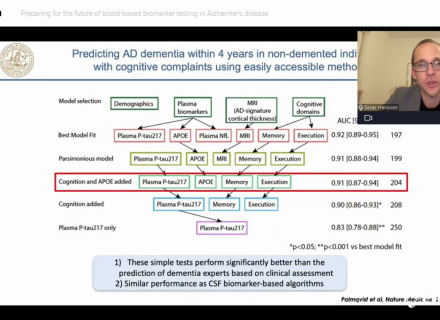
The combined use of CSF-Tau and CSF-β-amyloid(1-42) marker concentrations allows differentiation between Alzheimer’s disease (AD) and normal aging or other neurological diseases such as depression.1-6
Product number 81583
 Powered by Bioz
Powered by Bioz
-
Citations
The BIOZ badges associated with Fujirebio products include peer-reviewed citations derived from scientific studies using Fujirebio products. Please note that the peer-reviewed citations do not reflect the regulatory status of Fujirebio products. Users should refer to the specific product documentation and any (clinical) claims made therein in order to ensure compliant use. For each country or geographic region, users must verify the related regulatory status of the Fujirebio product.
-
Documentation
Browse regulatory documents for this product
Create a (free!) eServices account and start browsing all product documentation right away.
Multimedia
Watch product videos
Get a (free!) eServices account and benefit from full access to all our online resources.
Other documents
FileNeuroSig v6-0 macro for use with INNOTEST Neuro assays (vnd.ms-excel.sheet.macroEnabled.12, 214.10 kb)Extra informationThis macro is used with all Neuro INNOTEST assays for calculating the concentrations based on the OD values obtained by a plate reader.Get access to this section and more
Create a free eServices account now and instantly access multiple digital resources:
- Product documentation
- Selected scientific posters
- Product leaflets
- How-to videos and more…
-
Insights
Mar 31, 2026Integration of ADx NeuroSciences within Fujirebio unleashes a world of new possibilities
Fujirebio Europe N.V. will formally and fully integrate ADx NeuroSciences N.V. into its organization on April 1, 2026. This completes a process that...
Jul 23, 2025Fujirebio introduces its Neuro Expert Toolbox (NExT) at AAIC 2025
Fujirebio is introducing its Neuro Expert Toolbox (NExT) for the first time at AAIC 2025 (Alzheimer's Association International Conference®) in...
Nov 13, 2024Video - Alzheimer's awareness redefined
Follow the journey of the Sullivan family and leading Alzheimer’s Neurologist and Researcher Dr. David Greeley as they introduce and explain these...
-
Product inquiry
-
Related products









 and Lumipulse G β-Amyloid 1-40 Calibrators (231531)")
 and Lumipulse G β-Amyloid 1-42 Calibrators (230343)")
 and Lumipulse G pTau 181 Calibrators set (230367)")